A Medicare Stay of Enrollment can disrupt reimbursements, trigger claim rejection, and place your provider status at serious risk. Under CMS guidance like MLN13449, providers may face a temporary enrollment pause due to preliminary non-compliance status, missing Change of Information (COI) updates, or incomplete development request responses.
The good news is that a stay is not the same as revocation, and in many cases, it can be resolved before long-term damage occurs. Understanding how the 60-day pause works is critical for protecting revenue, maintaining Medicare participation, and preserving patient access to care.
From enrollment rebuttal rights to hardship exceptions and show cause orders, providers must act quickly and strategically to restore compliance. In this guide, we’ll explain exactly what a Medicare Stay of Enrollment means, why it happens, and how to resolve it before it escalates into revocation.
What Is a Medicare Stay of Enrollment?
A Medicare Stay of Enrollment is a temporary pause placed on a provider’s Medicare enrollment due to preliminary non-compliance status. Introduced under CMS guidance MLN13449, this action gives providers an opportunity to correct enrollment issues before CMS moves toward revocation.
Unlike revocation, a stay does not permanently remove a provider from the Medicare program. However, it immediately affects billing activity because claims submitted during the stay are rejected, not denied. This distinction matters because rejected claims are not processed for payment determination and may need to be resubmitted after compliance is restored.
In most cases, the stay lasts up to 60 days, depending on the type of non-compliance involved. CMS may use this interim action when providers fail to respond to enrollment requests, ignore documentation requirements, or delay Change of Information (COI) updates.
For providers, the key takeaway is simple: a stay of enrollment is a warning phase, not the final penalty. Fast corrective action can prevent escalation into revocation.
What Triggers a Medicare Stay of Enrollment?
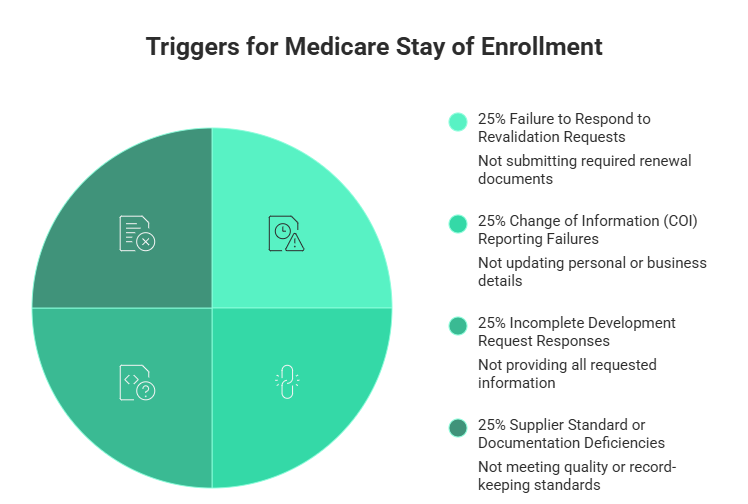
CMS may issue a Medicare Stay of Enrollment when a provider fails to meet enrollment or reporting requirements. These issues often begin as administrative oversights but can quickly evolve into serious compliance risks.
1. Failure to Respond to Revalidation Requests
Providers must periodically revalidate their Medicare enrollment information. Missing a revalidation deadline or submitting incomplete documentation may trigger a stay.
2. Change of Information (COI) Reporting Failures
CMS requires providers to report specific changes within designated timeframes. Delays involving ownership updates, practice locations, banking information, or managing employees can create compliance concerns and place the enrollment into a stayed status.
3. Incomplete Development Request Responses
Medicare Administrative Contractors (MACs) frequently issue development requests when additional documentation is needed. Providers who submit partial responses, incorrect files, or late documentation may face enrollment action.
Common mistakes include:
- Missing signatures
- Expired licenses
- Incorrect CMS forms
- Unverified EFT information
- Failure to respond within the deadline
4. Supplier Standard or Documentation Deficiencies
DMEPOS suppliers and healthcare organizations may also receive a stay due to operational deficiencies, record inconsistencies, or missing compliance documentation.
In many situations, providers are unaware of the issue until claims begin getting rejected. That’s why proactive enrollment monitoring is essential.
Understanding the Medicare 60-Day Pause
The Medicare 60-day pause is the temporary timeframe CMS uses to allow providers to resolve non-compliance issues before stronger enforcement actions occur.
During this period:
- Providers remain enrolled in Medicare
- Claims are rejected instead of denied
- Payments may be interrupted
- CMS expects corrective action immediately
The length of the stay depends on the underlying issue. For example, some revalidation-related problems may involve shorter correction windows, while unresolved COI issues can extend closer to the full 60 days.
This pause is not designed to punish providers permanently. Instead, CMS uses it as a corrective compliance mechanism. Providers who quickly submit accurate documentation and resolve deficiencies can often restore normal enrollment status before revocation becomes a possibility.
However, ignoring notices or delaying responses can increase the likelihood of escalated enforcement actions, including show cause orders or revocation proceedings.
For healthcare organizations, every day within the 60-day pause can impact cash flow, operations, and patient service continuity. Immediate action is the best strategy for minimizing disruption.
Claim Rejection vs Claim Denial: Why the Difference Matters
One of the most misunderstood parts of a Medicare Stay of Enrollment is the difference between a claim rejection and a claim denial. While the terms sound similar, they have very different financial and legal consequences for providers.
During a stay of enrollment, Medicare claims are typically rejected, not denied. A rejected claim is returned before full adjudication because the provider’s enrollment status is temporarily restricted. In contrast, a denied claim is processed and determined to be non-payable based on coverage or billing rules.
This distinction is important because rejected claims may still be resubmitted after the provider restores compliance. Denied claims, however, often require appeals or additional administrative action.
For healthcare organizations, rejected claims can create:
- Delayed reimbursements
- Revenue cycle disruptions
- Increased administrative workload
- Temporary cash flow issues
Providers should also understand that a rejected claim does not automatically mean fraud or misconduct. In many cases, the issue is tied to unresolved enrollment documentation or missing compliance updates.
The faster providers correct the non-compliance issue, the sooner claim submissions can resume normally.
How to Resolve a Medicare Stay of Enrollment Quickly
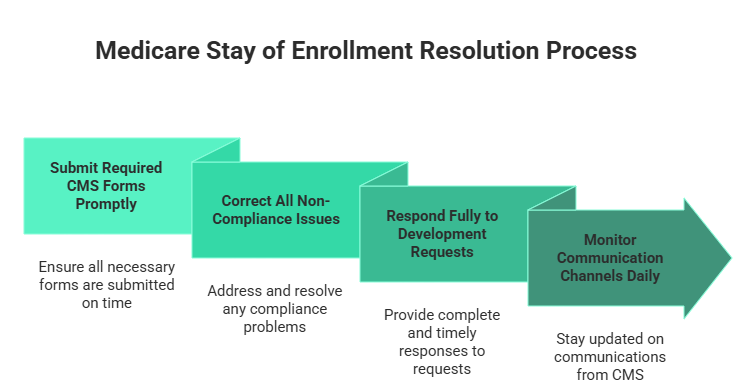
Resolving a Medicare Stay of Enrollment requires immediate and organized action. Delays can increase the risk of revocation and prolong reimbursement interruptions.
Submit Required CMS Forms Promptly
CMS may require updated enrollment documentation, including:
- CMS-855 enrollment forms
- CMS-588 EFT authorization
- Supporting ownership or licensing records
Every form should be reviewed carefully before submission to avoid additional deficiencies.
Correct All Non-Compliance Issues
Providers should identify the exact reason for the stay and address it directly. Common corrective actions include:
- Updating Change of Information (COI) records
- Completing overdue revalidation requirements
- Correcting inaccurate enrollment data
- Verifying operational addresses and ownership details
Respond Fully to Development Requests
A development request response should never be rushed or incomplete. MACs often escalate cases when providers fail to submit all requested documents within the required timeframe.
Best practices include:
- Responding before the deadline
- Including all requested attachments
- Keeping proof of submission
- Monitoring delivery confirmations
Monitor Communication Channels Daily
Many providers miss critical notices because emails go to spam folders or mail is routed incorrectly. Organizations should actively monitor:
- Email notifications
- Fax communications
- Physical mail
- PECOS account updates
Fast response times significantly improve the chances of resolving the stay before additional enforcement action occurs.
Enrollment Rebuttal Rights Explained
Providers placed under a Medicare Stay of Enrollment may have enrollment rebuttal rights depending on the circumstances surrounding the action.
A rebuttal allows providers to submit evidence explaining why CMS should reconsider the enrollment action. This process is especially important when providers believe the non-compliance determination was inaccurate or based on incomplete information.
When Can a Rebuttal Be Filed?
Rebuttals are typically time-sensitive and may require submission within a short deadline after receiving notice from CMS or the Medicare Administrative Contractor.
Providers should review all notices carefully to confirm:
- Filing deadlines
- Submission instructions
- Required supporting documentation
What Should Be Included in a Rebuttal?
Strong rebuttals focus on factual evidence rather than emotional arguments. Supporting documentation may include:
- Proof of timely submissions
- Updated compliance records
- Ownership verification documents
- COI reporting confirmations
- Communication logs with MACs
Common Rebuttal Mistakes
Many rebuttals fail because providers:
- Submit incomplete evidence
- Miss deadlines
- Ignore documentation requirements
- Fail to address the exact compliance issue
A well-prepared rebuttal can help prevent escalation and demonstrate good-faith compliance efforts to CMS.
Can a Stay of Enrollment Escalate Into Revocation?
Yes, a Medicare Stay of Enrollment can escalate into revocation if non-compliance issues remain unresolved. CMS uses the stay as an interim corrective action, but continued violations may trigger stronger enforcement measures.
Revocation risks increase when providers:
- Ignore CMS notices
- Miss response deadlines
- Submit inaccurate information
- Fail to correct enrollment deficiencies
- Repeatedly violate reporting requirements
Once revocation occurs, providers may lose Medicare billing privileges entirely and face re-enrollment restrictions. This can create long-term operational and financial damage for healthcare organizations.
Understanding Show Cause Orders
In serious cases, CMS may issue a show-cause order requiring the provider to explain why enrollment should not be revoked.
A show-cause order is a formal warning that signals elevated compliance concern. It often appears when CMS believes the provider has failed to meet Medicare enrollment obligations despite prior notices or corrective opportunities.
Providers receiving a show cause order should:
- Respond immediately
- Provide complete supporting documentation
- Correct all outstanding deficiencies
- Demonstrate active compliance efforts
Ignoring a show-cause order can significantly increase revocation exposure.
Key Risk Factors Providers Should Avoid
Several operational issues commonly increase enforcement risk, including:
- Poor documentation management
- Delayed COI reporting
- Lack of enrollment oversight
- Untracked revalidation deadlines
- Incomplete development request responses
Proactive compliance management is often the best defense against escalation.
Hardship Exceptions and Special Circumstances
In limited situations, providers may qualify for hardship exceptions or additional flexibility when responding to Medicare enrollment requirements.
CMS and Medicare Administrative Contractors may consider special circumstances that prevented timely compliance, especially when the provider can demonstrate good-faith efforts.
Potential hardship situations may include:
- Natural disasters
- Severe staffing shortages
- Technology failures
- Medical emergencies
- Loss of records due to unforeseen events
However, hardship considerations are not automatic. Providers must still communicate proactively and provide documentation supporting the request.
How to Strengthen a Hardship Exception Request?
A strong hardship explanation should include:
- A clear timeline of events
- Evidence of the disruption
- Corrective actions already taken
- Estimated resolution timeframe
- Proof of continued compliance efforts
Providers should avoid vague explanations or unsupported claims. Clear documentation improves credibility and increases the likelihood of consideration.
Even during hardship situations, delayed communication can still create compliance risks. Early engagement with the MAC is critical.
Best Practices to Avoid Future Medicare Enrollment Problems
Preventing a Medicare Stay of Enrollment is far easier than resolving one after claims begin getting rejected. Strong internal controls can reduce compliance exposure and improve operational stability.
Maintain a Change of Information (COI) Calendar
Track deadlines for reporting:
- Ownership changes
- Address updates
- Banking modifications
- Managing employee changes
Missing COI deadlines remains one of the most common enrollment issues.
Monitor Revalidation Dates Proactively
Providers should never wait for last-minute notices. Maintaining a centralized revalidation tracking system helps avoid missed deadlines and rushed submissions.
Centralize Development Request Responses
Assign a dedicated team or compliance lead to manage all CMS and MAC correspondence. Centralized oversight reduces the risk of incomplete or late responses.
Conduct Regular Enrollment Audits
Quarterly reviews can help identify:
- Outdated records
- Missing documentation
- Licensing inconsistencies
- Enrollment data errors
Internal audits also prepare organizations for future CMS reviews and reduce enforcement risks.
Assign Clear Compliance Responsibility
Many enrollment problems happen because responsibilities are unclear. Healthcare organizations should designate an enrollment compliance officer or responsible department to oversee Medicare reporting obligations.
A proactive compliance strategy not only reduces revocation risk but also protects revenue continuity and provider reputation.
Final Thoughts
A Medicare Stay of Enrollment is more than an administrative inconvenience. It can disrupt reimbursements, create operational instability, and place a provider’s Medicare participation at risk. However, unlike revocation, a stay offers providers an opportunity to correct non-compliance issues before facing more severe enforcement action.
Whether the issue involves Change of Information (COI) reporting failures, incomplete development request responses, or unresolved enrollment deficiencies, immediate action is essential. Providers who respond quickly, maintain organized documentation, and understand their enrollment rebuttal rights are in a far stronger position to restore compliance and protect revenue continuity.