As healthcare organizations continue expanding across state lines, remote physician supervision has become a critical part of modern care delivery. From telehealth networks to multi-location practices, providers are increasingly relying on supervising physicians who may never physically enter the same state as the patient or mid-level practitioner they oversee.
But while remote supervision creates flexibility and scalability, it also introduces a complex layer of credentialing, enrollment, and compliance challenges that many practices underestimate.
In reality, state medical board regulations, payer-specific supervision rules, incident-to billing requirements, and collaborative agreement obligations can all impact whether a supervising physician must be credentialed or enrolled locally.
Missing even one requirement can lead to denied claims, reimbursement delays, audit exposure, and costly compliance violations.
What Is Remote Physician Supervision in Multi-State Healthcare?
Remote physician supervision refers to a healthcare arrangement where a supervising physician oversees clinical services, treatment decisions, or operational responsibilities without being physically present at the same location as the provider delivering care. This model has become increasingly common with the rapid growth of telehealth services, multi-location practices, and expanding healthcare networks operating across multiple states.
In many healthcare organizations, supervising physicians remotely collaborate with nurse practitioners (NPs), physician assistants (PAs), and other mid-level practitioners to maintain continuity of care while supporting larger patient populations. However, remote supervision is not simply a virtual extension of traditional oversight. It introduces additional legal, credentialing, and payer compliance considerations that vary significantly depending on the state and insurance carrier involved.
Common Providers Involved in Remote Supervision
Remote supervision structures often include:
- Nurse Practitioners (NPs)
- Physician Assistants (PAs)
- Behavioral health clinicians
- Telehealth physicians
- Specialty consultants
- Rural healthcare providers
- Hospital outpatient departments
- Multi-state physician groups
Why Multi-State Supervision Creates Compliance Challenges
Healthcare organizations frequently assume that if a supervising physician holds a valid license, they can supervise providers nationwide without additional requirements. In reality, several layers of regulation may apply simultaneously, including:
- State medical board supervision laws
- Telehealth supervision requirements
- Payer-specific supervision rules
- Collaborative practice agreement mandates
- Medicare and Medicaid enrollment standards
- Facility credentialing requirements
Even when supervision occurs remotely through audio-video technology, practices must still verify whether the supervising physician requires local credentialing, payer enrollment, or additional registrations in the provider’s state.
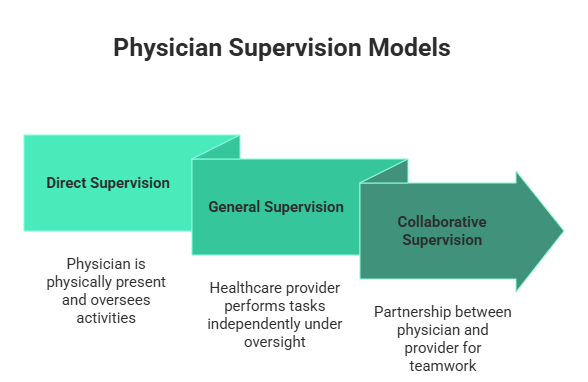
Types of Physician Supervision Models
Different supervision models carry different compliance obligations. Understanding the distinction is critical for avoiding billing and audit risks.
1. Direct Supervision
Direct supervision generally means the supervising physician must be immediately available to assist the rendering provider, even if not physically in the same room. Some states and payers now permit virtual availability through telecommunication technology.
This model is commonly associated with:
- Incident-to billing
- Medicare outpatient services
- Diagnostic testing supervision
- Certain telehealth encounters
2. General Supervision
Under general supervision, the physician provides overall direction and control, but their physical presence is not required during the service.
General supervision is often used for:
- Diagnostic procedures
- Chronic care management
- Ancillary healthcare services
- Administrative oversight structures
3. Collaborative Supervision
Collaborative supervision typically applies to nurse practitioners and advanced practice providers working under collaborative agreements established by state law.
These agreements may include:
- Prescriptive authority terms
- Chart review requirements
- Physician consultation expectations
- Delegated clinical responsibilities
- Billing oversight obligations
Important Difference Most Practices Overlook
One of the most misunderstood areas in remote supervision credentialing is the difference between state law and payer policy. A healthcare organization may technically satisfy state supervision requirements while still violating a commercial payer’s credentialing or enrollment rules.
For example:
- A state may allow remote oversight for mid-level practitioners
- But the payer may require the supervising physician to be locally enrolled
- Or require additional credentialing before claims can be reimbursed
This gap between legal compliance and payer compliance is where many practices experience denied claims, delayed reimbursements, and audit exposure.
Does a Remote Supervising Physician Need Local Credentialing?
The short answer is: sometimes yes, sometimes no. Whether a remote supervising physician requires local credentialing depends on several factors, including state regulations, payer contracts, billing structure, and the level of supervision being provided. There is no universal rule that applies across all states or insurance carriers, which is why multi-state supervision can quickly become complicated for healthcare organizations.
Key Factors That Determine Credentialing Requirements
Several variables influence whether a supervising physician must be locally credentialed:
- State medical board regulations
- Medicare supervision requirements
- Medicaid enrollment policies
- Commercial payer contracts
- Hospital or facility bylaws
- Scope-of-practice laws
- Type of healthcare services provided
- Billing methodology used by the practice
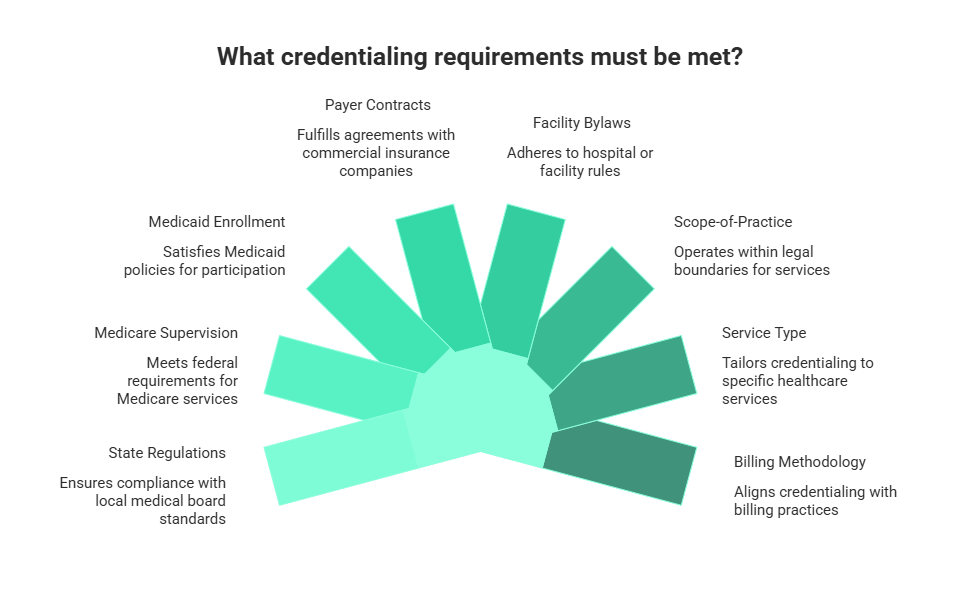
Because each payer and state operates differently, practices must evaluate supervision arrangements individually rather than relying on assumptions.
When Local Credentialing Is Usually Required
In many situations, remote supervising physicians must complete local credentialing and enrollment processes before services can legally or financially proceed.Common Scenarios Requiring Credentialing
Incident-To Billing Arrangements: If services are billed under the supervising physician’s National Provider Identifier (NPI), payers often require:
- Active enrollment
- Full credentialing
- Supervisory documentation
- Local participation status
This is especially important for Medicare incident-to billing structures.
Hospital or Facility Privileges: Hospitals and outpatient facilities may require supervising physicians to:
- Hold medical staff privileges
- Complete facility credentialing
- Maintain peer review eligibility
- Meet internal oversight standards
Medicaid Enrollment Requirements: Many state Medicaid programs require out-of-state provider enrollment even if the supervising physician never physically enters the state.
Failure to enroll properly can result in:
- Denied claims
- Payment recoupments
- Enrollment sanctions
- Delayed reimbursements
Commercial Insurance Participation: Commercial payers often impose stricter supervision and credentialing standards than state medical boards.
Payers may require:
- In-state credentialing
- Supervising physician enrollment
- Proof of collaborative agreements
- Telehealth-specific approvals
When Local Credentialing May Not Be Required
There are also situations where additional local credentialing may not be necessary.
Independent Billing Models: If nurse practitioners or physician assistants bill independently under their own credentials and payer contracts, the supervising physician may not require direct enrollment.
Non-Billing Advisory Supervision: Some physicians provide only administrative or educational oversight without participating in billing activities.
Examples include:
- Internal quality assurance
- Peer consultation
- Training oversight
- Non-clinical collaboration
Full Practice Authority States: Certain states grant nurse practitioners expanded or autonomous practice authority, reducing supervisory requirements.
In these cases:
- Formal physician oversight may be limited
- Collaborative agreements may not apply
- Supervising physician enrollment obligations may decrease
Why Practices Cannot Rely on Assumptions
A major compliance mistake occurs when organizations apply one state’s supervision rules across all operations. Multi-state healthcare models require careful review of each jurisdiction’s:
- Licensure standards
- Enrollment policies
- Telehealth supervision requirements
- Payer-specific supervision rules
- Mid-level practitioner laws
Even small oversight errors can trigger substantial revenue and compliance problems.
State Medical Board Rules That Impact Remote Supervision
Every state medical board establishes its own rules regarding physician supervision, delegation authority, and telehealth oversight. These regulations directly influence whether remote supervising physicians can legally oversee providers across state lines and whether additional credentialing or registration is required.
Because no national supervision standard exists, healthcare organizations operating in multiple states must navigate a highly fragmented regulatory environment. What is fully compliant in one state may create serious legal and billing issues in another.
Why State Medical Board Regulations Matter
State medical boards determine critical supervision standards, such as:
- Physician-to-provider supervision ratios
- Telehealth oversight permissions
- Prescriptive authority limitations
- Required chart review frequency
- Collaborative agreement obligations
- In-state physician availability standards
- Delegation of authority for mid-level practitioners
These rules affect not only clinical operations but also reimbursement eligibility and payer compliance.
Common Areas of State-by-State Variation
Supervision Ratios: Some states limit the number of mid-level practitioners a physician can supervise simultaneously.
Examples may include:
- Maximum NP supervision caps
- PA delegation limitations
- Rural exemption rules
- Specialty-specific restrictions
Exceeding these ratios may lead to:
- Regulatory penalties
- License investigations
- Invalid billing claims
- Credentialing complications
Chart Review Requirements: Certain states require supervising physicians to periodically review patient records managed by nurse practitioners or physician assistants.
Review standards can vary based on:
- Provider type
- Specialty
- Prescribing authority
- Telehealth involvement
Some states mandate:
- Monthly reviews
- Randomized chart sampling
- Signed documentation
- Quality assurance reporting
Telehealth Oversight Requirements: Remote supervision laws have evolved rapidly with telemedicine growth, but states continue to interpret virtual supervision differently.
Some jurisdictions allow:
- Real-time virtual supervision
- Audio-video physician availability
- Fully remote collaboration
Others still require:
- Physical proximity standards
- Periodic on-site visits
- In-state physician presence
- Additional telehealth registration
Examples of State-Level Differences
1. Texas
Texas historically maintained stricter supervision requirements for physician assistants and delegated prescriptive authority. Practices often face detailed documentation expectations and supervision ratio considerations.
2. California
California permits many telehealth supervision activities but maintains extensive provider documentation and collaborative oversight obligations depending on the practice structure.
3. Florida
Florida has expanded telehealth flexibility, but still requires providers to comply with licensing and payer enrollment standards when supervising across state lines.
4. Arizona
Arizona’s full practice authority environment for nurse practitioners reduces certain physician supervision obligations, though payer-specific rules still apply.
5. New York
New York frequently imposes more structured oversight and credentialing expectations for supervising arrangements involving mid-level practitioners.
One of the Biggest Compliance Misconceptions
A common mistake healthcare organizations make is assuming that if telehealth services are allowed in a state, remote supervision is automatically permitted under the same rules. In reality, telehealth laws and supervision laws are often regulated separately.
For example:
- A physician may legally provide telehealth services in a state
- But still fail to meet supervision standards for incident-to billing
- Or fail payer enrollment requirements for collaborative oversight
This distinction is critical for maintaining compliant multi-state operations.
Multi-State Licensure vs Credentialing: What’s the Difference?
One of the biggest causes of compliance confusion in remote physician supervision is misunderstanding the difference between licensure, credentialing, and provider enrollment. Many healthcare organizations assume these terms mean the same thing, but each serves a completely different purpose in multi-state healthcare operations.
Multi-State Licensure vs Credentialing vs Enrollment
| Category | Purpose | Issued By | Main Function |
| Multi-State Licensure | Grants legal authority to practice medicine | State medical board | Allows physicians to legally practice in a state |
| Credentialing | Verifies qualifications and competency | Hospitals, payers, healthcare organizations | Confirms provider eligibility for participation |
| Provider Enrollment | Approves billing participation | Medicare, Medicaid, and commercial payers | Enables reimbursement for healthcare services |
What Multi-State Licensure Covers
Multi-state licensure allows physicians to legally practice medicine across multiple jurisdictions. This process is regulated by each individual State medical board.
Licensure requirements often include:
- Medical education verification
- Background checks
- State application approvals
- Continuing medical education compliance
- DEA registration requirements
Some physicians use the Interstate Medical Licensure Compact (IMLC) to accelerate licensing across participating states.
What Credentialing Covers?
Credentialing focuses on evaluating a provider’s qualifications, training, work history, and professional standing. Healthcare organizations and insurance payers use credentialing to determine whether a physician meets participation standards.
Credentialing reviews may include:
- Board certification verification
- Malpractice history
- Work experience review
- Hospital affiliations
- Sanctions screening
- CAQH profile validation
What Provider Enrollment Covers?
Provider enrollment connects physicians to insurance networks and government healthcare programs for reimbursement purposes.
Enrollment may involve:
- Medicare registration
- Medicaid participation
- Commercial payer contracting
- Telehealth network approvals
- Out-of-state provider enrollment
Why the Difference Matters in Remote Supervision?
A supervising physician can face compliance issues if even one layer is missing.
| Scenario | Possible Risk |
| Licensed but not credentialed | Facility or payer rejection |
| Credentialed but not enrolled | Claim denials |
| Enrolled but lacking state licensure | Regulatory violations |
| Telehealth approved but not supervision compliant | Billing audits |
Common Misconception Healthcare Practices Make
A physician having multi-state licensure does not automatically satisfy:
- Payer-specific supervision rules
- Hospital credentialing requirements
- Incident-to billing standards
- Medicaid enrollment obligations
- Telehealth supervision requirements
Practices must evaluate all three areas separately to maintain compliant remote supervision structures.
Out-of-State Provider Enrollment Explained
Out-of-state provider enrollment is one of the most overlooked components of remote supervision compliance. Even when a supervising physician is fully licensed and credentialed, many payers still require formal enrollment before claims can be processed correctly.
This issue becomes especially important in telehealth and multi-state healthcare operations where supervising physicians oversee providers remotely across state lines. Without proper enrollment, practices may experience denied claims, reimbursement delays, or retrospective payment recoupments.
Why Out-of-State Enrollment Matters
Insurance companies and government healthcare programs use enrollment systems to verify provider participation and reimbursement eligibility.
Without proper enrollment, organizations may face:
- Non-payable claims
- Out-of-network billing problems
- Retroactive claim denials
- Compliance investigations
- Delayed revenue cycles
Types of Enrollment Remote Supervising Physicians May Need
| Enrollment Type | Purpose | Common Requirement |
| Medicare Enrollment | Federal reimbursement participation | Required for Medicare billing |
| Medicaid Enrollment | State Medicaid participation | Often state-specific |
| Commercial Payer Enrollment | Insurance network participation | Required for contracted claims |
| Telehealth Enrollment | Virtual care reimbursement approval | Required by some payers |
Medicare Enrollment Requirements
Medicare supervision rules often require supervising physicians to maintain active enrollment when services are billed under their oversight.
This is especially relevant for:
- Incident-to billing
- Outpatient services
- Telehealth supervision
- Diagnostic testing oversight
Practices must also ensure:
- Correct practice location reporting
- Updated reassignment records
- Accurate NPI information
- Active PECOS registration
Medicaid Enrollment Complexity
Medicaid enrollment rules vary significantly by state. Some states require out-of-state supervising physicians to enroll even when they never physically treat patients within the state.
Common Medicaid requirements include:
- State-specific applications
- Fingerprinting
- Background screening
- Additional disclosure forms
- Site verification processes
Commercial Insurance Enrollment Challenges
Commercial payers frequently impose their own supervision and credentialing standards that exceed state medical board requirements.
Payers may require:
- Supervising physician participation agreements
- Telehealth-specific approvals
- Delegated credentialing verification
- Mid-level practitioner linkage documentation
Common Enrollment Mistakes Practices Make
| Mistake | Potential Consequence |
| Assuming licensure equals enrollment | Claim denials |
| Missing Medicaid registration | Reimbursement delays |
| Using an incorrect billing provider | Audit exposure |
| Failing to update payer records | Contract violations |
| Overlooking telehealth enrollment rules | Payment rejections |
Why Enrollment Delays Create Revenue Problems
Enrollment processing timelines can vary from several weeks to several months, depending on the payer and state. During this time, claims may remain unpaid or denied entirely.
This often affects:
- Expanding telehealth organizations
- Multi-state physician groups
- Hospital-owned practices
- Behavioral health networks
- Large provider onboarding initiatives
Healthcare organizations that proactively manage out-of-state provider enrollment typically experience fewer disruptions and stronger revenue cycle performance.
Telehealth Supervision Requirements
Telehealth has transformed how supervising physicians oversee patient care, but remote supervision still comes with strict compliance obligations. While many states expanded telehealth flexibility in recent years, healthcare organizations must still comply with supervision laws, credentialing requirements, and payer-specific billing standards.
What Telehealth Supervision Means
Telehealth supervision involves physicians overseeing healthcare services remotely using approved communication technology.
This may include:
- Real-time audio-video oversight
- Remote consultation availability
- Virtual collaborative supervision
- Telemedicine-based physician support
- Remote chart review processes
Key Areas That Affect Telehealth Supervision Compliance
| Compliance Area | Why It Matters |
| State Licensure | Determines legal authority to practice |
| Telehealth Registration | Required in some states |
| Payer Rules | Controls reimbursement eligibility |
| Supervision Documentation | Supports audit protection |
| Technology Standards | Ensures HIPAA compliance |
Telehealth Supervision vs Traditional Supervision
| Traditional Supervision | Telehealth Supervision |
| On-site physician presence | Remote physician availability |
| Physical office oversight | Audio-video oversight |
| Local practice structure | Multi-state operations |
| Easier documentation verification | Higher compliance scrutiny |
| Standard credentialing process | Additional telehealth approvals |
Common Telehealth Supervision Risks
Healthcare organizations often encounter problems such as:
- Supervising without proper enrollment
- Using unsupported billing models
- Violating payer-specific supervision rules
- Failing to document physician availability
- Ignoring state telemedicine restrictions
Collaborative Agreement Billing and Compliance Risks
Collaborative agreements define the working relationship between a supervising physician and a mid-level practitioner, such as a nurse practitioner or physician assistant. In many states, these agreements are legally required before certain services can be provided or billed.
For multi-state practices, collaborative agreement compliance becomes more complicated because each state has different supervision standards, documentation requirements, and billing expectations.
Common Elements Included in Collaborative Agreements
- Scope of practice
- Prescriptive authority
- Chart review frequency
- Physician availability
- Delegated responsibilities
- Supervision protocols
Collaborative Agreement vs Independent Practice
| Collaborative Practice | Independent Practice |
| Physician oversight required | Minimal physician involvement |
| Formal agreement needed | The agreement may not apply |
| Higher billing scrutiny | More provider autonomy |
| State supervision laws apply | Reduced supervision restrictions |
Billing Risks Practices Often Missed
| Compliance Issue | Potential Consequence |
| Expired agreement | Claim denials |
| Missing signatures | Audit exposure |
| Incorrect supervising physician | Billing violations |
| Outdated state-specific language | Compliance penalties |
Incident-To Billing in Multi-State Supervision
Incident-to billing allows services performed by certain non-physician providers to be billed under a supervising physician’s NPI. While this can increase reimbursement, it also creates strict supervision and credentialing obligations.
Remote supervision makes incident-to billing more complex because practices must satisfy both payer requirements and state supervision laws.
Core Incident-To Billing Requirements
| Requirement | Purpose |
| Supervising physician involvement | Supports billing eligibility |
| Active physician enrollment | Allows reimbursement |
| Proper supervision level | Maintains compliance |
| Credentialed supervising physician | Prevents denials |
Common Incident-To Billing Mistakes
- Billing under a non-enrolled physician
- Missing supervision documentation
- Assuming virtual supervision always qualifies
- Ignoring payer-specific supervision rules
- Using incident-to billing across states without verifying compliance
Incident-To Billing vs Independent Billing
| Incident-To Billing | Independent Billing |
| Billed under physician NPI | Billed under provider NPI |
| Higher reimbursement potential | Standard reimbursement |
| Strict supervision required | More provider flexibility |
| Higher audit risk | Lower supervision exposure |
Why Remote Supervision Creates Risk
Some payers permit virtual supervision, while others still require stricter oversight standards. If supervision rules are not met, healthcare organizations may face:
- Denied claims
- Payment recoupments
- Medicare audits
- Compliance investigations
Practices should verify payer policies before using incident-to billing in multi-state telehealth environments.
Common Compliance Mistakes in Multi-State Physician Supervision
Many healthcare organizations assume that state licensure alone is enough for remote supervision. In reality, payer enrollment, credentialing, and billing compliance all play separate roles.
Some of the most common mistakes include:
- Billing under non-enrolled supervising physicians
- Expired collaborative agreements
- Incorrect incident-to billing
- Missing supervision documentation
- Ignoring payer-specific supervision rules
- Failing to update credentialing records
- Supervising beyond state-approved provider limits
These issues can result in claim denials, payment recoupments, audit exposure, and operational delays. Practices that perform routine compliance reviews are better equipped to manage multi-state supervision successfully.
Need Help Managing Multi-State Provider Credentialing?
Managing remote supervision, payer enrollment, and multi-state licensure can quickly become challenging for healthcare organizations expanding across state lines. From telehealth supervision requirements to incident-to billing compliance, even small credentialing gaps can create reimbursement and audit risks.
Working with an experienced credentialing partner helps practices streamline provider enrollment, maintain compliance, and reduce administrative delays across multiple payers and states.
Visit DR Credentialing to learn more about provider credentialing, telehealth enrollment, and remote supervising physician support.
Conclusion
Remote physician supervision offers flexibility and scalability for modern healthcare organizations, but it also creates complex credentialing and compliance responsibilities. Multi-state licensure alone is not enough to satisfy payer enrollment, supervision documentation, and billing requirements.
Healthcare practices must carefully evaluate state medical board regulations, payer-specific supervision rules, collaborative agreement obligations, and incident-to billing standards before expanding remote supervision operations. A proactive credentialing and compliance strategy helps reduce denied claims, avoid audit exposure, and support long-term operational growth.