
Many providers and billing teams are facing unexpected disruptions in 2026 due to Medicare non-billing deactivation. Under updated CMS enforcement, providers who do not submit a Medicare claim for 6 consecutive months can have their billing privileges deactivated. This rule has led to a noticeable increase in inactive provider records, especially among low-volume specialists and newly enrolled providers.
Recent CMS compliance updates indicate that billing inactivity is now one of the most common triggers for deactivation, alongside enrollment noncompliance. Internal CMS data presented in 2026 shows that inactivity-based actions have risen significantly since the rule update, with thousands of providers affected annually. In parallel, CMS reported over 3,300+ entities placed on the preclusion list between 2022 and 2025, reflecting broader enforcement efforts to maintain program integrity.
This issue directly impacts revenue and operations. Providers cannot bill Medicare during deactivation, and no retroactive payments are allowed for services delivered in that period. Even a short lapse can result in permanent revenue loss. This guide explains the 6-month rule, causes of inactivity, financial risks, and the CMS provider enrollment reactivation process, with clear steps to help providers, coders, and RCM teams maintain compliance and avoid disruption through expert provider enrollment and credentialing services.
Medicare non-billing deactivation 2026: The 6-Month Rule Explained
This section explains how the 6-month Medicare billing rule works in 2026. It outlines triggers, enforcement purposes, and which providers face the highest risk.
What Triggers Non-Billing Deactivation
Under CMS updates, providers may lose billing privileges if no Medicare claim is submitted for 6 consecutive months. This applies across individual and group enrollments.
Key triggers include:
- No Part B claims submitted within 6 months
- Claims created but not transmitted to Medicare.
- Repeated claim rejections with no resubmission
- Enrollment is active, but billing activity is at zero
Why CMS Enforces the 6-Month Rule
CMS applies this rule to maintain accurate enrollment records and reduce inactive billing identifiers.
Primary reasons include:
- Remove unused or dormant billing privileges.
- Lower risk of improper billing activity
- Maintain current provider enrollment data.
- Improve oversight of active Medicare participants.
Who Is at Highest Risk
Certain provider groups face higher exposure due to billing patterns or operational gaps.
High-risk categories:
- Specialists with low Medicare patient volume
- New providers delaying first claim submission
- Practices relying on secondary insurance before Medicare billing
- Providers with frequent claim denials or coding errors
- Clinics with gaps in revenue cycle tracking
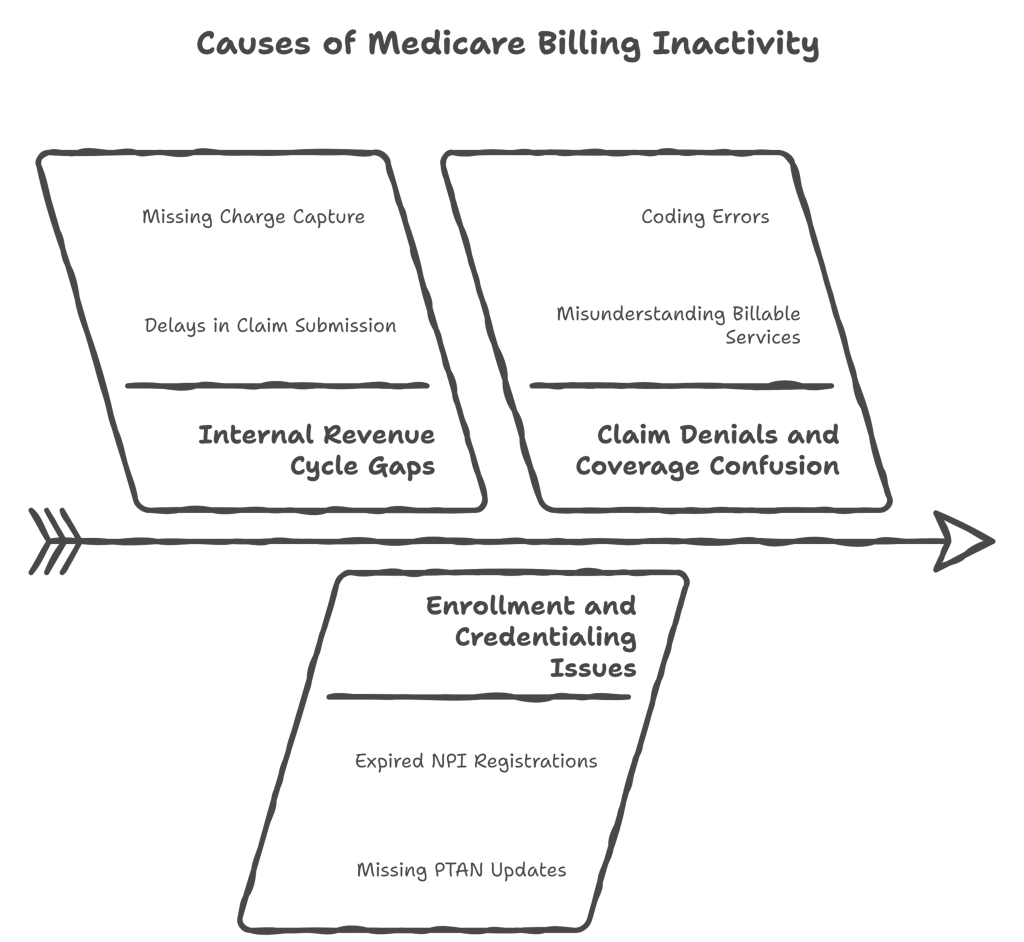
Common Causes Behind Medicare Billing Inactivity
Billing inactivity can trigger Medicare non-billing deactivation in 2026. This section explains the main causes, helping providers and billing teams prevent deactivation and maintain active enrollment.
Internal Revenue Cycle Gaps
Internal gaps in revenue cycle management can lead to prolonged inactivity. Key issues include:
- Delays in submitting claims to Medicare
- Missing charge capture or incomplete documentation
- Lack of follow-up on rejected or denied claims
Enrollment and Credentialing Issues
Inactive or outdated enrollment records increase deactivation risk. Common factors include:
- Expired or pending NPI registrations
- Missing updates in PTAN information
- Delays in completing CMS-required provider documentation
Claim Denials and Coverage Confusion
Frequent claim denials or confusion over Medicare coverage can reduce submitted claims. Contributing factors:
- Misunderstanding which services are billable under Part A or Part B
- Denials due to coding errors or prior authorization issues
- Lack of proper follow-up on denied claims
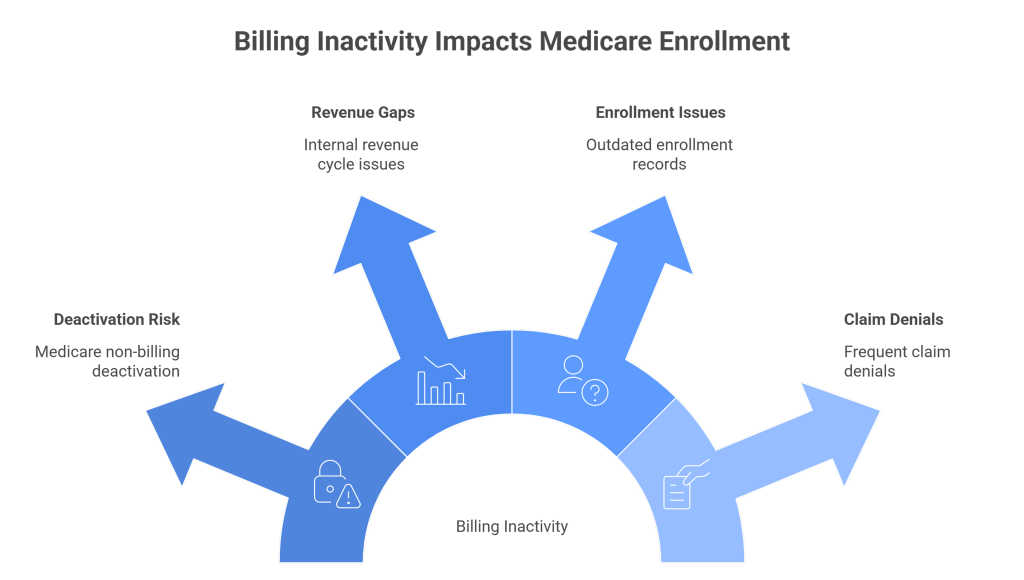
Financial and Compliance Impact of Deactivation
Deactivation under Medicare non-billing deactivation 2026 has tangible consequences for providers and billing teams. It can halt reimbursements, disrupt operations, and expose practices to compliance risks. Understanding these impacts is essential for maintaining smooth revenue cycles and protecting provider privileges.
Revenue Loss and Billing Gaps
Providers who are deactivated stop receiving Medicare payments immediately. This interruption affects both pending claims and future services. Specialists with occasional Medicare patients are particularly vulnerable, as even a short 6-month lapse can lead to significant financial shortfalls. Practices must track claim activity closely to ensure no revenue is lost due to inactivity.
Key financial consequences include:
- Unpaid claims for services already delivered
- Delayed reimbursements for ongoing treatments
- Potential write-offs for services during the inactive period
Operational Disruptions
Billing interruptions directly impact administrative workflows. Staff may spend extra hours completing reactivation forms, submitting documentation, or following up on suspended claims. This increased workload can reduce efficiency across the revenue cycle and create delays in patient account management.
Operational impacts include:
- Idle staff time while resolving NPI billing status
- Delays in submitting and reconciling claims
- Increased administrative burden for practice managers and billing teams
Compliance and Audit Risk
Deactivation raises compliance risks because CMS closely monitors inactive providers, which is why many practices rely on Healthcare Audit Protection Services for ongoing oversight. Failure to respond to deactivation notices, update, or maintain updated records can trigger audits. Retroactive claims may require thorough documentation to be approved, placing additional pressure on billing staff.
Key compliance considerations include:
- Timely response to CMS deactivation letters
- Complete documentation of services during inactive periods
- Accurate PTAN records for Medicare PTAN reactivation 2026
CMS Provider Enrollment Reactivation Process
Understanding the CMS provider enrollment reactivation process is critical for providers impacted by the Medicare non-billing deactivation in 2026. This process allows healthcare professionals to restore billing privileges and resume submitting claims. Following the correct steps ensures faster reactivation and minimizes financial and compliance risks.
Many providers use professional Physician Enrollment Services to speed up reactivation and avoid processing delays.
Steps to Reactivate Billing Privileges
Reactivating billing privileges begins with reviewing the CMS deactivation letter and identifying the required documentation. Providers must complete the relevant forms, most commonly Form CMS-855A, CMS-855B, or CMS-855I, depending on provider type, and submit them to the local Medicare Administrative Contractor (MAC).
Key steps include:
- Collecting all supporting documentation for NPI and PTAN verification
- Filling out the appropriate CMS enrollment form accurately
- Submitting forms via fax, mail, or the PECOS online system
- Confirming receipt with the local MAC to avoid processing delays
Reactivation Timelines and Effective Dates
After submitting reactivation forms, CMS examines the application, which can take 30-60 days depending on workload and document completion. Coverage is retroactive in some cases, especially when a provider submits paperwork within 6 months of deactivation. Knowing effective dates is crucial for properly reconciling claims and avoiding revenue loss.
Important points regarding timelines:
- Standard review time: 4–8 weeks for most provider types
- Retroactive coverage may be available up to 6 months from reactivation submission.
- Providers should track submission and approval dates closely to align with claim-filing deadlines.
Common Errors That Delay Reactivation
Errors in form submission or missing documentation are the most frequent causes of delays in restoring Medicare billing privileges. Incomplete NPI records, outdated PTAN information, or misfiled CMS forms can trigger additional requests from the MAC, further extending the reactivation timeline.
Frequent issues include:
- Incorrect or incomplete provider demographic information
- Missing licenses, certifications, or attestation signatures
- Failure to respond promptly to MAC follow-up requests
CMS Deactivation Letter Response and Rebuttal Process
Receiving a CMS deactivation letter can be alarming for providers affected by the Medicare non-billing deactivation of 2026. Understanding how to respond and when to appeal is critical to restoring billing privileges efficiently. A structured approach ensures compliance and reduces revenue gaps.
How to Respond to a Deactivation Letter
The first step is reviewing the CMS deactivation letter carefully. It details the reason for inactivation, usually due to no Medicare claims submitted for six consecutive months. Providers must gather supporting documentation to confirm billing activity or explain inactivity.
Key actions include:
- Verify the dates and services cited in the letter against practice records.
- Complete the required CMS forms, typically CMS-855A/B/I, depending on provider type.
- Include attachments such as claims history, contracts, or proof of service provision.
- Submit the response via fax, mail, or the PECOS portal to the appropriate Medicare.
- Administrative Contractor (MAC)
Rebuttal Process and Deadlines
If a provider disputes the deactivation, CMS allows a formal rebuttal process. Providers must submit their explanation and evidence within the deadline specified in the letter, typically 30 days from receipt. The rebuttal must clearly address the inactivity reason and provide supporting documents.
Important steps and considerations:
- Draft a concise, factual rebuttal addressing all points in the deactivation letter.
- Attach verifiable evidence, such as Medicare claims or patient service logs.
- Ensure submission within the stated deadline to avoid automatic denial of the rebuttal.
- Keep copies of all correspondence for compliance and audit purposes
When to Escalate the Issue
Escalation is necessary if the rebuttal is denied or if CMS does not respond within the expected timeframe. Providers may contact the MAC supervisor, request a reconsideration, or involve the CMS regional office. Escalation ensures that unresolved deactivations do not block claims submission indefinitely.
Situations that warrant escalation:
- Lack of response from the MAC beyond standard review periods (usually 30–60 days)
- Denial of rebuttal despite providing complete documentation
- Complex cases involving multiple provider locations or NPI/PTAN inconsistencies
Preventing Medicare Non-Billing Deactivation
Proactive measures can help providers avoid Medicare non-billing deactivation in 2026. Implementing routine billing checks, strong internal controls, and staff compliance training reduces the risk of losing billing privileges. Prevention minimizes revenue loss and operational disruptions.
Monthly Billing Activity Checklist
Regularly monitoring Medicare billing activity ensures providers meet the 6-month Medicare billing rule. A monthly checklist helps identify inactive NPIs before CMS initiates deactivation.
Key items to track:
- Confirm all Medicare claims are submitted and processed on time.
- Review rejected or denied claims and take corrective action
- Track patient visits for Medicare beneficiaries to ensure claims are created.
- Maintain a log of submitted claims by provider and date
Internal RCM Controls
Internal revenue cycle management (RCM) controls support continuous Medicare billing activity. These processes ensure all claims are processed and billed correctly, preventing unintended inactivity.
Essential RCM controls:
- Automate reminders for providers with low Medicare patient volume
- Implement routine audits for pending or rejected claims.
- Maintain a centralized record of all Medicare claims for verification.
- Establish a workflow for tracking inactive NPIs and notifying responsible staff.
Staff Training and Compliance Monitoring
Well-trained staff is critical for maintaining an active Medicare billing status. Training ensures everyone understands the CMS provider enrollment reactivation process and the importance of continuous billing activity.
Best practices include:
- Educate billing staff on the 6-month rule and deactivation triggers.
- Conduct quarterly compliance reviews of NPIs and PTAN activity.
- Provide updates on CMS policy changes affecting Medicare billing.
- Assign staff to monitor and report any gaps in Medicare claim submissions.
Medicare Billing Lifecycle and Compliance Timeline (2026)
Understanding the full Medicare billing lifecycle helps providers maintain active status and avoid Medicare non-billing deactivation in 2026. Compliance checkpoints at each stage reduce operational risks and protect billing privileges.
Key Compliance Milestones
Tracking compliance milestones ensures providers meet CMS requirements and avoid unintentional inactivity. These milestones mark essential deadlines for claims submission, documentation, and NPI activity.
Key milestones include:
- Monthly claims submission and verification for all Medicare patients
- Timely resolution of rejected or denied claims within CMS deadlines
- Quarterly internal audits of billing activity and documentation
- Annual review of provider enrollment information and PTAN status
Lifecycle Risks and Control Points
At each stage of the billing lifecycle, risks may emerge that could trigger deactivation. Identifying control points allows for timely corrective action and safeguards Medicare privileges.
Critical control points:
1. New patient intake: Ensure Medicare eligibility verification and proper documentation
2. Claim preparation: Validate CPT/HCPCS codes, modifiers, and NPI usage
3. Claim submission: Confirm all claims are transmitted and acknowledged by MACs
4. Post-submission review: Monitor claim status, rejections, and denials to prevent gaps
Conclusion
Maintaining continuous Medicare billing activity is essential to prevent Medicare non-billing deactivation in 2026. Providers, coders, and RCM teams must follow the 6-month rule, monitor claims, and ensure accurate enrollment records to protect revenue and compliance.
Proactive internal controls, staff training, and timely responses to CMS notices reduce operational disruptions and safeguard billing privileges. Staying informed of CMS updates allows healthcare practices to maintain uninterrupted Medicare participation and minimize financial risk.
FAQs
What is Medicare non-billing deactivation 2026?
It is the CMS process that deactivates providers who do not submit a Medicare claim for six consecutive months, halting billing privileges.
Who is most at risk for deactivation?
Low-volume specialists, new providers, and practices with frequent claim denials or gaps in revenue cycle tracking face the highest risk.
How can providers reactivate their Medicare billing privileges?
Providers must submit the appropriate CMS enrollment forms (CMS-855A/B/I) with supporting documentation through PECOS or their local MAC.
What common errors delay reactivation?
Incomplete forms, outdated PTAN or NPI records, and missing licenses or attestation signatures often cause delays in restoring billing privileges.
How can practices prevent deactivation?
Implement monthly billing checks, internal RCM controls, and staff compliance training to maintain continuous Medicare billing activity.



